
Clinical Excellence
Pantai Hospital Kuala Lumpur is committed to upholding the highest standards of clinical integrity in all aspects of patient care.
Here, we highlight our dedication to clinical performance, which encompasses our commitment to delivering quality care, patient safety, and positive outcomes. We understand that achieving clinical excellence requires a multi-faceted approach, which is why we continually invest in the latest technologies, invite the most skilled medical professionals to join us, and improve our processes and procedures.
Our goal is to provide our patients with the best possible outcomes and experiences while ensuring that we maintain our commitment to clinical integrity.
- Patient Safety and Quality Data
Our Commitment to Patient Safety and Quality
Patient safety is simply defined by the World Health Organization as “the prevention of errors and adverse effects to patients associated with health care”.
At Pantai Hospital Kuala Lumpur, patient safety is paramount. Every day we work together to deliver effective and efficient care while protecting our patients from harm.
We have created a culture where emphasis is given to patient safety, ultimately increasing awareness and trust as healthcare providers via communication and leadership. Our main components of patient care delivery listed below are continuously reviewed, analyzed, and improved.
- Timely and effective access to care
- Safe patient care following International Patient Safety Goals (IPSG)
- Adherence to evidence-based practices which results in better patient outcomes and lower costs of care for consumers
- Integrated clinical and operational data
International Patient Safety Goals (IPSG)
- Patient Identification
- Effective Communication
- Safety of High Alert Medications
- Safe Surgery
- Reducing the risk of healthcare associated infections
- Reducing the risk of patient harm resulting from falls
Pantai Hospital Kuala Lumpur prides on our excellent patient safety measures and outcomes as a result of our strict infection control protocols.
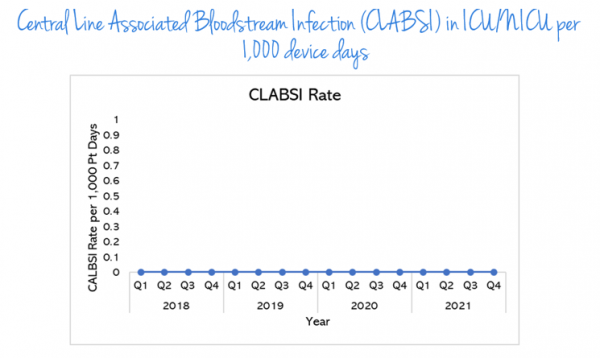
Central line Associated Bloodstream infections (CLABSI) in ICU/nICU per 1,000 device days
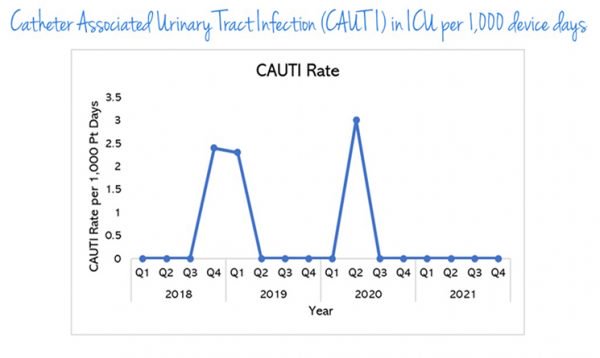
Catheter Associated Urinary Tract Infection (CAUTI) in ICU per 1,000 device days
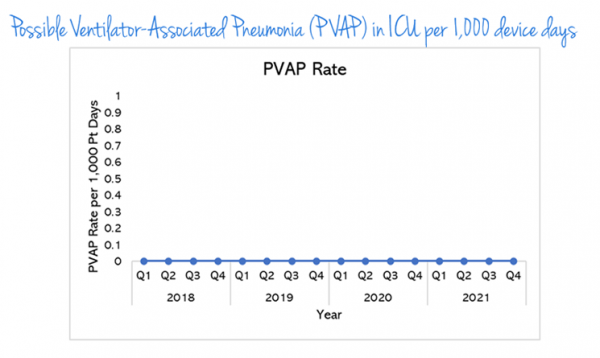
Possible Ventilator-Associated Pneumonia (PVAP) in ICU per 1,000 device days
Possible Ventilator-Associated Pneumonia (PVAP) in ICU per 1,000 device days
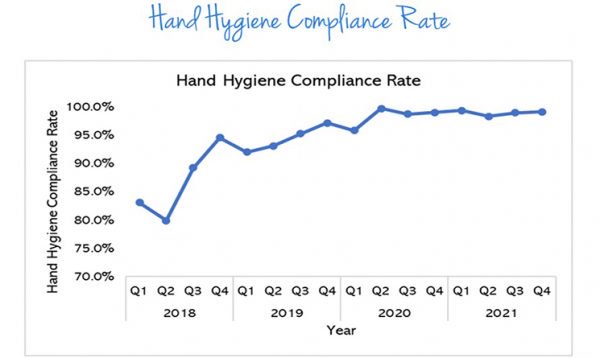
Hand Hygiene Compliance Rate
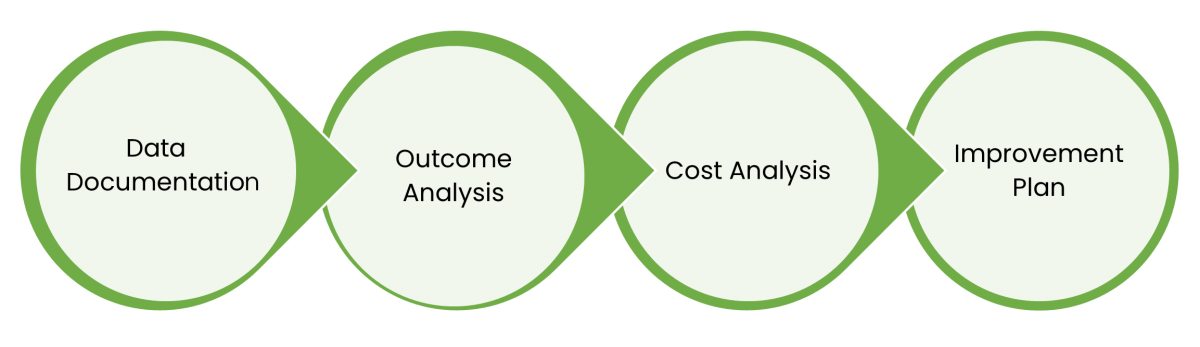
- Value Driven Outcomes (VDO)
- Antimicrobial Stewardship (AMS) Data
- Breast Imaging Score (BI-RADS)




.webp?sfvrsn=20763f7d_19)
.webp?sfvrsn=f2a2c343_9)